For the last several months (or longer), after a round of Uceris to tamp down some smoldering inflammation, I’ve ventured more into “whole foods plant based” diet territory, in an effort to forestall the need for more steroids or Humira or similar. I’m now in remission and for the last several months I’ve been eating beans (usually navy beans in soup, or mixed in with brown rice pasta) several days a week for the last six months. I began testing out beans – at first with trepidation – after reading the study I posted on this blog earlier (about navy beans and white kidney beans in particular). I had good results with them so I kept eating them.
In the past, after a flare, I’d eat in fear – fearful that the “wrong” thing could kick of an inflammatory spiral. Now, while I certainly have my avoid list (featured at least partially on this blog), in general, by eating a 80-90% whole foods plant based diet (no processed foods), no alcohol and no sugar, so far I’m remaining solidly in remission (while continuing with my maintenance meds).
As I’ve been typing this, I’ve been eating pumpkin seeds in the shell…
The exceptions to the “plant based” approach are fish (cod or salmon for lunch 2-3 x’s a week), kefir, and a small amount of low fat cheese (a few times a week).
This is something that comes up repeatedly in a variety of studies and anecdotal reports from fellow Colitis patients (many of which are featured on this blog):
“Fiber-rich foods act as fuel for the “good” bacteria that live in the gut and produce short-chain fatty acids, which are critical for an efficient immune response.
Eating high-sugar diets and decreasing intake of fiber feeds “bad” microbes, such as E. coli, that are associated with inflammation and a defective immune response.
Madsen’s study showed that the mice on the high-sugar diet had greater intestinal tissue damage and a defective immune response. These problems were alleviated when their diet was supplemented with short-chain fatty acids normally produced by good bacteria.”
Many years ago, a doctor, “my” gastro. at the time (who I liked, but I’ve moved away since then), suggested I give curcumin a try. Back then, as far as I know, there weren’t different formulations featuring variations intended to maximize delivery (e.g. black pepper, lipids, etc.).
The doctor warned that there might be side effects such as bright yellow urine and even a curry like odor. Still, I went ahead and grabbed a bottle from Whole Foods. After a few days, I did notice the atomic urine and my stomach felt unsettled and -what a shock – after three days I didn’t see any benefits so I stopped taking it.
I can’t remember what prompted me to look into it (curcumin) again a couple of years ago, besides looking to maximize anti-inflammatory food (and possibly, supplement) intake. Now that I’m thinking of it, it may have been prompted by an effort to avoid needing to take a biologic (and Anti-TNF) and while looking for foods that naturally lower TNF (something I don’t know anything about – I’m not a scientist), I learned that curcumin is Anti-TNF.
I then set out to research which type of curcumin would be best for colitis, since now days, there are different formulations (for example some cross the blood brain barrier and might be useful for say, Alzheimer’s and some do not). I also looked into what doses were used in medical studies.
Ultimately, I tried a couple of different kinds and started with the lowest dose at first and built up. The formula I settled on is Meriva which uses a lipid (sunflower oil) as a carrier to help the body absorb the curcumin. Other products use black pepper to increase potency but I read it can’t irritate your stomach. I also found research data indicating that certain formulations are more potent than others. If you refer to the study I linked above, you can see what dosages were used in research studies. Right now I use this and take two in the morning and one around dinner time: https://www.pureencapsulations.com/curcumasorb.html
Remember: I am not a doctor! I’m a colitis patient and this what I do with the knowledge of my doctor. Always ask your doctor before taking anything, including supplement.
What I do know is curcumin can thin your blood and potentially increase potency of meds. It has also been associated with anemia. I became anemic after a flare while taking high doses of curcumin. I don’t know if that was the reason but it’s important to be aware of this potential side effect among others, including kidney stones. I think I even read about someone who died from taking too much curcumin. So with anything med or supplement, proceed with caution and consult your doctor.
Anecdotally, my colitis symptoms seem to have improved (less frequent flares, inflammation more mild overall) since I’ve been taking it (for at least 2 years now). Ask your own doctor if it’s something you want to explore for yourself.
And… a “shout out” to the gastro. from years back who first mentioned curcumin to me. In hindsight, I wish I’d have stuck with it longer than a few days!
The difference though, is back then, there was pretty much just one formula, nothing like Meriva another innovations that we have now, so the body could just not process it well – or make use of it. Now, as numerous legit. evidenced based studies show, such as those that I’ve linked to above, there are different curcumin products that appear promising for various ailments, including colitis.
In past blog post, I mentioned that years ago, when I was diagnosed, I asked the gastro. at the time if I could keep drinking coffee. He was dismissive and said something to that effect that, “It doesn’t matter what you eat.” Back then and even now, the belief was, “Food doesn’t cause Colitis.” Meanwhile though, there are numerous studies, especially in the last few years, showing how diet and the health of one’s microbiome has a cause & effect relationship with digestive diseases. A new study (in mice) shows, for example, that eating fried food basically demolishes your gut and worsens UC (what a surprise…): https://www.sciencedaily.com/releases/2019/08/190823094825.htm
And interestingly, a number of Colitis patients have self-treated through strict dietary intervention(Kenny Honnas – What I ate to Heal): https://www.youtube.com/watch?v=7Lo2I1gUYfg
And lastly (for this blog post), there’s a link between a high sugar diet and Colitis induction – A high-sugar diet rapidly enhances susceptibility to colitis via depletion of luminal short-chain fatty acids in mice: https://www.nature.com/articles/s41598-019-48749-2
This might be a Rosetta Stone: rapidly enhances susceptibility to colitis via depletion of luminal short-chain fatty acids
Looking back at the period of my life preceding my diagnosis. I was in grad. school and had a fairly high-stress lifestyle. For the most part, I thought I had a healthy diet but there are products I consumed back then that I would not now (for instance, Almond Milk, which contains Carrageenan, and is featured on the “avoid” list on this blog).
Something I recall eating back then (idiotically), was something called a chocolate orange. It’s a baseball sized sphere of chocolate and it breaks apart into slices that a sensible person would eat sparingly (e.g. one slice once in a while). But not me…I ate the whole thing at once. And soon after, there was blood in my stool, so to speak. Did the chocolate orange cause my colitis? Was it that plus genetic susceptibility plus other dietary and/or lifestyle factors? In my opinion the chocolate orange was, at a minimum, not a good idea and based on some of the science I posted above MAY have played a role. Also on the ingredient list of the chocolate orange is “milkfat” something contained in other candies and also linked to fueling “bad” gut bacteria. Subsequently, chocolate products have induced flares for me, in particular the ones containing “milkfat.” Obviously I never eat chocolate anymore and avoid added sugar in general (which is pro-inflammatory anyway),
With respect to short-chain fatty acids, what seems to have had really good results for me, is eating foods that cultivate scfa’s and avoiding ones that deplete them. Much info. on this blog covers this ground (what to eat / what to avoid).
So why does much medical literature still say that diet doesn’t cause Colitis or “everyone is different”, eat what you want? Yes, it’s true that we all have particular foods that we can or cannot eat and what leads to IBD is still mysterious and unknown, but it also seems to be complete b.s. to ignore the aggregation of data indicating that optimizing one’s diet can produce significant benefits. Or the numerous studies that keep pointing to benefits of fiber, SCFA’s, and a whole foods plant based diet (or Mediterranean diet). It might be a frustrating and painstaking process, figuring out what works for you over a course of months, or my case, years. But it’s worth it.
What I’ve seen online though, is probably what doctors often face when they suggest to someone with high blood pressure/ cholesterol/ type 2 diabetes, etc. that they adhere to a diet proven to reverse disease… Most people want a painless quick fix… they want to keep downing the onion rings and cheese burgers and beer (or whatever), AND be perfectly healthy or symptom free. I see comments online from some fellow IBD’ers that are similar.
So, can your dietary choices lead to colitis? I don’t know if it’s the “one thing,” but it certainly can degrade or cultivate a healthy microbiome, something that supports a good digestive health whether you have IBD or not. For me, I believe that eating the chocolate orange played a role. Then again, maybe I would’ve gotten Colitis anyway sooner or later. Who knows…
In any case, plenty of research shows that yes, a poor diet can increase your odds of getting UC, and a “good” one can minimize them (as well as yield improvements – or not – for people who already have it). Whether or not you want to accept this is up to you.
This year, always seeking to optimize my diet, I am prob. 80% plant based, at least. The rest is Mediterranean diet (fish and some yogurt) and I’ve been enjoying the longest period of remission I’ve had in ten years.
As I’ve said, I’m not a doctor. I’m someone who has had Colitis for over two decades and have basically been running experiments on myself for that time – an articulate guinea pig…
Gut microbiota plays a crucial role in triggering, maintaining, and exacerbating IBD. Specific microbes can be overrepresented in IBD while others seem to be protective. A decrease in microbial biodiversity has been found in mucosa and feces of IBD patients, together with an increase of fungi. Pre- and probiotics could represent a valid armamentarium to modulate gut microbiota and, probably, to cure IBD. Current evidences, however, show a clear clinical efficacy of some families of probiotics only in pouchitis and ulcerative colitis but not in Crohn’s disease. This efficacy has been prevalently associated to mild disease and seems to have a better role in maintenance of remission compared to induction of remission. Further studies are necessary to better characterize the exact role of probiotics in IBD, their specific mechanisms of actions, including a direct effect on mucosal homeostasis or healing. Since probiotics are becoming a legitimate therapeutic option, it is necessary to determine which probiotic strains have the greatest efficacy, whether they are more effective alone, or in conjunction with other pro- or prebiotics, and what is their half-life in the gastrointestinal tract. On the base of these data, frequency of administration and dose could be exactly calculated.
When I was younger, I dreaded going to the pharmacy to pick up four large boxes (a month supply) of Mesalamine Suspension Enemas. At the time, the pharmacy (a major chain) used flimsy plastic bags that were essentially transparent, fully allowing other customers to read “Rectal” and “Enema’ conveniently printed in block letters on all sides of each box. Because of the way the boxes were printed, you couldn’t just say, adjust the way you carried the bag to conceal it. I think I took to bringing my own bags or a large backpack and putting the boxes into that as soon as I could at the counter. Now, the same chain uses paper bags, but I’m not particularly fond of leaving a drug store with grocery sized bads of meds either.
The truth is, at this point, I don’t care. Yes, it’s a little annoying when I “call in” a refill of Mesalamine Suppositories and the pharm tech accidentally fills the enemas. What’s changed for me, is now I get it that no one cares. There’s nothing to be embarrassed about.
Setting aside that aspect, I also never had any aversion to using UC rectal meds in the first place. I was first prescribed them in my twenties, and found they helped (I’ve also used hydrocortisone enemas, suppositories, and most recently foam). In fact, mesalamine rectal products (susp. enemas and suppositories) have been a mainstay of my regimen for years. I have a study somewhere (that I can confirm in vivo with myself) that – for me- using a Mesalamine Enema once a week has provided really good results for what gastros refer to as “maintenance”.
Apparently, not all patients are open to using rectal meds. I get it. It’s gross. And if you’re younger and dating, I could see that it could be a source of stress or embarrassment. It need not be and the truth is, for me, my flaring colitis was inhibiting my dating and sex life, not the use of rectal meds. And in any case, the administration of the med does not take that long, particularly once you get used it.
And rectal meds for UC seem like common sense. They treat the problem area topically – at least the parts of the colon they’re able to reach.
So dear readers, if you’re shy or wary about trying these products , and if your doctor thinks they could help you, they’re worth trying. For me, apart from that they work, I vastly prefer them to some other options since they have pretty minimal side effects.
And now days, I no longer have to fantasize about paying a stranger to retrieve my Mesalmine enemas for me from the pharmacy. I just go in with my backpack, politely pay the pharm tech., and leave.
This post is somewhat rambling, prompted after coming across a study (link below) about Walnuts perhaps being preventative for Colitis.
For years, nuts (mainly almonds) were something I’d eat with a caution and obviously not while in a flare. Perhaps I’ll delve into this in another post but somewhere along the line I came to understand that, anecdotally at least, patients with Colitis were having good results with sunflower seeds and cooked spinach. In any case, at some point many years ago, I began eating Sunflower Seed Butter (unsweetened and w/o added sodium), and stuck to nut butters over nuts.
Now, after a short course of Uceris in June to tackle some mild yet smoldering inflammation, I’ve optimized my diet (again), and as I’ve been feeling good have been experimenting with foods such as nuts. Knowing how beneficial walnuts are supposed to be, I’ve been eating a small amount now, daily, for months. I’ve also added other varieties like macadamias. So far, no issues at all.
I think a lot of IBD’ers live in fear that some food item could send them into a flare. And who can blames us? A lot of foods or questionable ingredients (many of which I’ve covered on this blog and will cover in the future) can wreak havoc on our digestive systems and bodies.
That’s why it’s important to have your “avoid” list (which takes time, though trial and error as well as research), and also to be informed about nutritional basics, such as the difference between soluble and insoluble fiber.
Over time though, you can develop a fear-based eating pattern. Eventually you figure out a safe list and discover you’re cycling through the same meals. That is not great for nutrition or health generally, and it’s not good for IBD. Eating diverse foods (e.g. variety of veg., fruits, complex carbs) is what results in a diverse microbiome). So…perhaps in an effort to avoid a flare, you avoid your potential triggers, and stick to a limited “safe” list. In turn, your nutrition suffers and low and behold you slide into a flare…
When not in a flare, I don’t dig into pizzas and fries and greasy food (for example) so I can eat like a “normal” person. I like eating healthy as it is, but for me it’s also important to eat things that will prolong remission (and certainly not put me at risk for another).
Which brings me back to walnuts. Whenever I see a research study like this, I make note of it and if it’s reasonably convenient, I try to incorporate it into my diet. I’ve done that with walnuts and now, as I said, I eat them daily. My point is that, for a long time, I avoided nuts in their whole form, thinking they’d be a problem. At this point, more or less in remission, they aren’t.
Am I saying you should eat walnuts? No. What I’m saying is, just as you exercise caution with what you consume, you should also be careful about backing yourself into a corner food-wise where you end up avoid/cutting items that could be helping you.
“Interestingly, biomarkers of colon barrier integrity (crypt height, mucus content, cell proliferation and goblet cell number) were enhanced in BB vs. NB-fed mice, suggesting added benefits attributable to unique BB components (e.g., phenolics). Overall, NB and BB improved baseline colonic microenvironment function by altering the microbial community structure and activity and promoting colon barrier integrity and function; effects which may prove beneficial in attenuating gut-associated diseases.”
“…both WK and DK bean-supplemented diets enhanced microbial-derived SCFA metabolite production, gut barrier integrity and the microbial defensive response in the healthy colon, which supported an anti-inflammatory phenotype during colitis. Collectively, these data demonstrate a beneficial colon-function priming effect of bean consumption that mitigates colitis severity.“
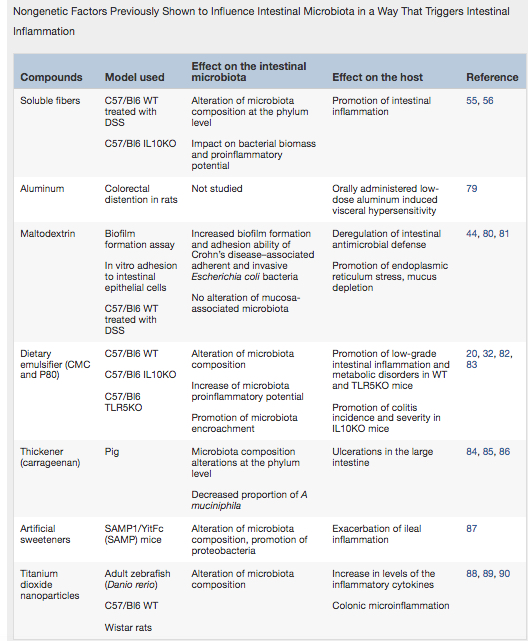
Notice that Caraageenan, previously addressed on this blog, is featured on the list. I personally avoid foods (and toothpaste!) that contain it. In case I didn’t mention it earlier, it can also be found in some beers. Anyway, please check out this article and the chart inside: